






Glaucoma is a chronic, progressive optic neuropathy and remains a leading cause of irreversible blindness worldwide. Large, well-controlled clinical trials, including the Early Manifest Glaucoma Trial and the Advanced Glaucoma Intervention Study, have consistently demonstrated that lowering intraocular pressure (IOP) reduces the risk of structural and functional disease progression.1,2 As such, IOP reduction remains the central therapeutic target across all stages of glaucoma.
In routine clinical practice, however, achieving sustained IOP control remains challenging. Topical pharmacotherapy, while effective, is limited by issues of adherence and tolerability. Numerous studies have shown that a significant proportion of patients fail to administer medications as prescribed, leading to fluctuating IOP and increased risk of progression.3 Furthermore, chronic exposure to preserved topical agents is associated with ocular surface disease, inflammation, and tear film instability, which may negatively affect patient comfort, visual quality, and surgical outcomes.4
Laser trabeculoplasty has gained increasing acceptance as a nonincisional treatment option and is frequently used earlier in treatment algorithms.5,6 Nevertheless, variability in response and limited durability remain important considerations. Minimally invasive glaucoma surgery has further expanded procedural options; however, these interventions remain intraocular and are often dependent on concurrent cataract surgery.7
Collectively, these limitations highlight a gap between available therapies and the need for treatments that are noninvasive, repeatable, and compatible with long-term disease management. As the field shifts toward earlier intervention, there is increasing interest in approaches that preserve tissue and maintain future treatment flexibility.

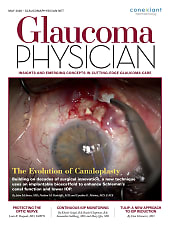
Figure 1. Clinical photograph demonstrating proper placement of the TULIP transducer at the limbus. The probe tip (~3 mm) is covered with a sterile latex sheath. A wire speculum maintains separation of the upper and lower eyelids.
Technology Overview
Therapeutic ultrasound to lower intraocular pressure (TULIP) is an investigational, noninvasive, low-power ultrasound platform designed to modulate aqueous humor dynamics without thermal ablation or structural tissue disruption. The procedure is performed in an office using a handheld transducer applied circumferentially at the limbus under topical anesthesia. The treatment interface is designed to ensure consistent contact and reproducible energy delivery.
Unlike high-intensity focused ultrasound systems used for cyclodestruction,8 TULIP operates at acoustic intensities that are intended to avoid thermal coagulation and structural tissue damage. No incisions, intraocular instrumentation, or implanted devices are required. The procedure is designed to be efficient, well tolerated, and compatible with standard clinical workflows.
The conceptual distinction between TULIP and traditional therapies lies in its emphasis on physiologic modulation rather than tissue destruction. The system is intended to influence biologic processes involved in aqueous outflow and regulation. The mild stressors of the vibrational and mild thermal elevation point to a possible sonobiomodulation effect.

Figure 2. TULIP handheld ultrasound transducer with tapered ~3 mm tip designed for precise limbal placement. The probe is used with a sterile latex sheath during treatment.
Mechanistic Rationale for Low-Power Ultrasound
The biologic effects of ultrasound at low intensities are mediated primarily through mechanical stimulation rather than thermal injury.9 These mechanotransductive effects influence cellular behavior by altering membrane permeability, cytoskeletal organization, and intracellular signaling pathways.
Within the trabecular meshwork, ultrasound exposure has been associated with changes in extracellular matrix composition and cellular contractility, which may enhance aqueous humor outflow. Effects on Schlemm’s canal endothelial cells and collector channels may further contribute to improved outflow facility.
In contrast to cyclodestructive procedures, which rely on coagulative necrosis of the ciliary body to reduce aqueous production, low-power ultrasound appears to act through nonablative modulation of cellular function. This distinction is particularly relevant in a chronic disease requiring repeated intervention over time.
Emerging data also suggest that ultrasound may influence neuroautonomic pathways involved in aqueous humor regulation. Although these mechanisms remain under investigation, they provide a potential explanation for observations that extend beyond localized tissue effects and may represent an additional dimension of ultrasound biomodulation.

Figure 3. TULIP console used to set and monitor treatment parameters, including energy output and duration, enabling controlled and reproducible ultrasound delivery.
Early Clinical Experience and Aravind Studies
Early clinical evaluation at Aravind Eye Hospital provides important preliminary insight into the safety and biologic activity of low-power ultrasound biomodulation. In a small study (n=15), treatment with TULIP was associated with a mean IOP reduction of approximately 25.8% compared to control. Reductions were observed consistently across follow-up visits, suggesting a sustained physiologic response within the limits of the study duration.
Importantly, no evidence of thermal injury or structural tissue disruption was identified on slit-lamp or gonioscopic examination. The absence of clinically significant inflammation is consistent with the nonablative energy profile of the device.
Structural and functional assessments were also performed. Optical coherence tomography demonstrated stability of retinal nerve fiber layer thickness, and standard automated perimetry did not show progression of visual field indices during the observation period. Although these findings are limited by sample size and follow-up duration, they suggest that ultrasound biomodulation does not adversely affect retinal structure in the short term.
A notable finding was a reduction in IOP in the untreated contralateral eye. This bilateral effect has been described in other neuromodulatory contexts and raises the possibility of centrally mediated or neuro-autonomic mechanisms. Although exploratory, this observation is mechanistically plausible given the known systemic effects of ultrasound signaling.
The procedure was performed under topical anesthesia in an outpatient setting and was well tolerated. No serious adverse events, including hypotony, persistent inflammation, or vision-threatening complications, were reported. Larger studies with longer follow-up are required to confirm these findings and further define safety and durability.
Biomarker analysis (n=9) further supported a biologic response, demonstrating changes in cytokine expression associated with extracellular matrix remodeling and cellular signaling. These findings are consistent with mechanotransductive effects but do not yet establish a direct causal relationship with clinical outcomes.
Safety and Repeatability
Safety is a critical consideration for any new glaucoma therapy, particularly those involving energy delivery to ocular tissues. High-intensity ultrasound systems used for cyclodestruction achieve IOP reduction through targeted tissue coagulation and are associated with known risks, including inflammation and hypotony.8
By contrast, TULIP utilizes lower acoustic intensities designed to avoid structural disruption. The absence of clinically significant inflammation or tissue injury in early clinical experience supports a tissue-preserving approach.
This nonablative profile has implications for repeatability. Because ultrasound biomodulation does not rely on cumulative tissue damage, repeat treatments may be feasible without compromising ocular integrity. This may be particularly relevant in glaucoma, where long-term management often requires multiple interventions. In addition, preservation of conjunctival and scleral architecture may maintain future surgical options, an important consideration in patients who may eventually require filtering or tube-based procedures.
Clinical Positioning in the Treatment Algorithm
Within contemporary glaucoma management, TULIP is being investigated as a noninvasive procedural option that may complement existing therapies. In early disease, it may represent an alternative for patients in whom adherence or ocular surface toxicity limits the effectiveness of topical therapy. As interventional-first paradigms continue to evolve, nonpharmacologic options are increasingly being considered earlier in the disease course.
In patients with inadequate control following laser or medication escalation, TULIP offers a mechanistically distinct option that does not preclude subsequent surgical intervention. In moderate disease, it may serve as an adjunctive therapy or a bridge to incisional procedures, although this role remains to be defined in controlled studies.
The observation of bilateral IOP reduction introduces a potentially important consideration. If validated, this finding may influence treatment paradigms, particularly in patients with asymmetric disease. At present, however, it should be considered hypothesis-generating.
Impact on Medication Burden and Quality of Life
Reducing medication burden remains an important goal in glaucoma care. Procedural interventions that lower IOP have the potential to reduce reliance on chronic topical therapy, thereby improving ocular surface health and patient comfort.
For elderly patients and those with limited dexterity, minimizing daily medication requirements may simplify treatment regimens and improve adherence. Improvements in quality of life associated with reduced treatment burden may also contribute to better long-term disease control.
Although these potential benefits are conceptually aligned with noninvasive procedural approaches, they require confirmation in prospective clinical studies.
Future Directions
Prospective clinical trials will be essential to define the magnitude and durability of IOP reduction achieved with TULIP, as well as optimal retreatment intervals and safety across glaucoma subtypes.
Comparative studies with SLT and other interventional modalities will further clarify its role within treatment algorithms. In addition, continued investigation into the biologic mechanisms underlying ultrasound-mediated modulation of aqueous humor dynamics may help refine patient selection and optimize treatment parameters.
Long-term studies will be particularly important to assess durability of effect, repeatability, and integration into chronic disease management strategies.
Conclusion
TULIP represents an investigational, noninvasive sonobiomodulatory approach to IOP reduction. By emphasizing physiologic modulation rather than tissue destruction, the platform aligns with evolving trends toward earlier, repeatable, and tissue-preserving intervention.
Early clinical observations demonstrate biologic activity with a favorable short-term safety profile. Continued clinical investigation will determine its ultimate role within the expanding spectrum of glaucoma therapies. GP

References
1. Heijl A, Bengtsson B, Oskarsdottir SE. Prevalence and severity of undetected manifest glaucoma: results from the early manifest glaucoma trial screening. Ophthalmology. 2013;120(8):1541-1545. doi:10.1016/j.ophtha.2013.01.043
2. Kim J, Dally LG, Ederer F, et al. The Advanced Glaucoma Intervention Study (AGIS): 14. Distinguishing progression of glaucoma from visual field fluctuations. Ophthalmology. 2004;111(11):2109-2116. doi:10.1016/j.ophtha.2004.06.029
3. Friedman DS, Okeke CO, Jampel HD, et al. Risk factors for poor adherence to eyedrops in electronically monitored patients with glaucoma. Ophthalmology. 2009;116(6):1097-1105. doi:10.1016/j.ophtha.2009.01.021
4. Jaenen N, Baudouin C, Pouliquen P, Manni G, Figueiredo A, Zeyen T. Ocular symptoms and signs with preserved and preservative-free glaucoma medications. Eur J Ophthalmol. 2007;17(3):341-349. doi:10.1177/112067210701700311
5. Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Laser in Glaucoma and Ocular Hypertension (LiGHT) Trial: six-year results of primary selective laser trabeculoplasty versus eye drops for the treatment of glaucoma and ocular hypertension. Ophthalmology. 2023;130(2):139-151. doi:10.1016/j.ophtha.2022.09.009
6. Garg A, Vickerstaff V, Nathwani N, et al. Primary selective laser trabeculoplasty for open-angle glaucoma and ocular hypertension: clinical outcomes, predictors of success, and safety from the Laser in Glaucoma and Ocular Hypertension Trial. Ophthalmology. 2019;126(9):1238-1248. doi:10.1016/j.ophtha.2019.04.012
7. Sharma A, Tijerina JD, Bitrian E. Minimally invasive, maximally impactful: minimally invasive glaucoma surgery and the changing glaucoma landscape. Curr Opin Ophthalmol. 2024;35(5):409-414. doi:10.1097/ICU.0000000000001077
8. Marques RE, Ferreira NP, Sousa DC, et al. High intensity focused ultrasound for glaucoma: 1-year results from a prospective pragmatic study. Eye (Lond). 2021;35(2):484-489. doi:10.1038/s41433-020-0878-0
9. Baek H, Pahk KJ, Kim H. A review of low-intensity focused ultrasound for neuromodulation. Biomed Eng Lett. 2017;7(2):135-142. doi:10.1007/s13534-016-0007-y